Colchicine-Macrolide Interaction Checker
Check Your Medication Safety
This tool identifies dangerous interactions between colchicine and antibiotics based on current medical guidelines.
Important: This tool doesn't replace medical advice. Always consult your doctor before changing medications.
Recommended actions
Immediate action needed: If you experience muscle pain, weakness, nausea, or unusual fatigue, contact your doctor immediately.
When you take colchicine for gout or heart inflammation, you’re not just managing pain-you’re walking a tightrope. One wrong drug combo, and that small pill can turn deadly. The biggest danger? Mixing it with common antibiotics like clarithromycin or erythromycin. It’s not just a theoretical risk. Real people have died from it. And it’s happening more often than you think.
Why This Interaction Is So Dangerous
Colchicine is a tiny molecule with a massive risk profile. It works by blocking cell division in inflamed tissues, which is why it’s so effective for gout flares and pericarditis. But here’s the catch: your body barely knows how to handle it. Only 30-50% of a dose even makes it into your bloodstream because your liver and gut break it down before it can do its job. That’s where CYP3A4 comes in-a liver enzyme that metabolizes colchicine. And then there’s P-glycoprotein (P-gp), a cellular pump that kicks colchicine out of cells before it builds up to toxic levels. Now, add a macrolide antibiotic like clarithromycin. It doesn’t just fight bacteria. It slams the brakes on both CYP3A4 and P-gp. The result? Colchicine doesn’t get broken down. It doesn’t get pumped out. It just piles up. In some cases, plasma levels can quadruple. Toxicity kicks in at just 3.3 ng/mL. With this combo, you can hit 10 ng/mL or higher-without even trying.Not All Macrolides Are the Same
Here’s where things get messy. Not every macrolide is equally dangerous. Clarithromycin? High risk. Erythromycin? Moderate. Azithromycin? Almost none. Why? Because their chemical structures, while similar, interact differently with enzymes and transporters. Clarithromycin blocks CYP3A4 with an IC50 of 1.6 μM-meaning it’s powerful. It also inhibits P-gp at 12.7 μM. Erythromycin? Its CYP3A4 inhibition is weaker (Ki=30 μM), and it barely touches P-gp. Azithromycin? It doesn’t meaningfully inhibit either. A 2022 study of over 12,000 patients found that those taking clarithromycin or erythromycin with colchicine had more than double the risk of toxicity. But those on azithromycin? No increased risk. That’s not a small difference. It’s the difference between a safe antibiotic choice and a potential ER visit.Real Cases, Real Consequences
The FDA’s adverse event database has 147 reports of colchicine toxicity linked to macrolides between 2015 and 2020. Sixty-three percent involved clarithromycin. Twenty-eight percent involved erythromycin. And in a 2019 case series, 12 patients developed rhabdomyolysis, neutropenia, or multi-organ failure after taking standard colchicine doses with clarithromycin. Three of them died. Emergency medicine doctors report seeing this more than rheumatologists. Why? Because when someone comes in with chest pain or pneumonia, they’re often prescribed clarithromycin. If they’re also on colchicine for heart disease or gout, no one checks. Electronic health records rarely flag it well. Patients don’t think to mention their gout pill. And many don’t even know they’re taking colchicine-it’s just a daily tablet they’ve been on for years.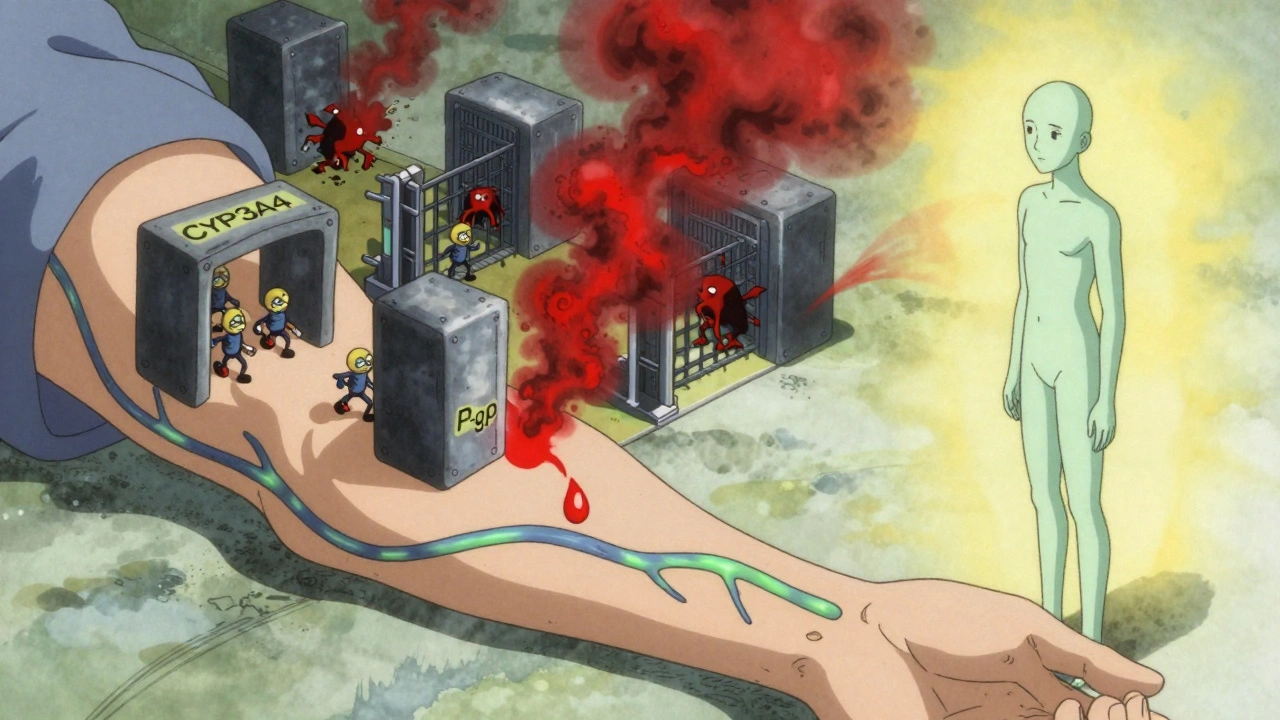
Who’s at Highest Risk?
It’s not just anyone. Certain people are sitting ducks:- People with kidney problems-colchicine is cleared by the kidneys, and even mild impairment doubles toxicity risk
- Older adults-liver and kidney function decline with age
- Those on multiple meds-especially statins, calcium channel blockers, or antifungals that also inhibit CYP3A4 or P-gp
- People taking supplements like St. John’s wort or grapefruit juice-both inhibit CYP3A4
What Should You Do?
If you’re on colchicine, here’s your action plan:- Never take clarithromycin or erythromycin without talking to your doctor first. Even a 5-day course can be dangerous.
- Ask for azithromycin instead. It works just as well for most infections and doesn’t interact.
- If you must take a high-risk macrolide, your colchicine dose must be cut in half-and even then, it’s risky. Monitor for muscle pain, weakness, nausea, or unusual fatigue.
- Check all your meds. Even over-the-counter drugs like some antifungals or heart pills can cause the same interaction.
- Get tested if you’re high-risk. Some hospitals can measure colchicine levels in your blood. If yours is above 2.5 ng/mL, you’re in danger.
Why Don’t More Doctors Know This?
A 2021 study found that 43% of internal medicine residents couldn’t identify high-risk drug combos involving colchicine. That’s not their fault. The alerts in electronic systems are often buried. Some systems only warn if you’re taking two strong inhibitors-but miss the fact that colchicine is already a narrow-window drug. Even worse, many doctors assume that because colchicine has been around for centuries, it’s safe. But modern usage has changed. In 2010, it was mostly for gout. Now, thanks to FDA approvals for heart disease and pericarditis, prescriptions have jumped 217% since 2010. That means more people are taking it-and more are getting exposed to macrolides.What’s Being Done?
Some hospitals are finally catching up. Epic’s 2023 update added a tiered alert system for colchicine interactions. In a multi-center trial, it cut inappropriate prescribing by 63%. That’s huge. Researchers are also working on a new version of colchicine-COL-098-that doesn’t rely on P-gp or CYP3A4. Early trials show it’s 92% less likely to interact with clarithromycin. If it works, this could be a game-changer. Meanwhile, genetic testing is emerging. A 2023 study found that two common gene variants-CYP3A5*3/*3 and ABCB1 3435C>T-predicted 78% of toxicity cases. Soon, your DNA might tell your doctor whether you’re at high risk before you even take a pill.Bottom Line: Don’t Guess. Ask.
Colchicine is essential. For many, it’s the only thing keeping them out of the hospital. But it’s not harmless. When paired with the wrong antibiotic, it becomes a silent killer. If you’re on colchicine and your doctor prescribes an antibiotic, ask: "Is this azithromycin? If not, is it safe with colchicine?" If they hesitate, push back. Bring up the FDA’s black box warning. Show them the data. Your life might depend on it.There’s no reason to wait for a crisis. This interaction is predictable. Preventable. And far too common.
Ali Bradshaw
December 6, 2025 AT 03:40Just had my doc switch me from clarithromycin to azithromycin last month after I mentioned I was on colchicine. I didn’t even know there was a risk. Thanks for laying this out so clearly-this could save someone’s life.
luke newton
December 7, 2025 AT 12:05People who don’t read the fine print deserve what they get. I’ve been on colchicine for 12 years and never had an issue-until some dumbass pharmacist didn’t check my med list. Now I carry a laminated card. You’re not special. You’re not immune. Stop being lazy.
an mo
December 9, 2025 AT 06:15Colchicine toxicity is a classic CYP3A4/P-gp pharmacokinetic cascade. The clinical implications are non-trivial, especially in polypharmacy cohorts with renal insufficiency. The FDA’s AE database underreports by at least 40% due to coding inaccuracies. We need mandatory EHR alerts tied to pharmacogenomic data-not just drug-drug interactions.
Lynette Myles
December 9, 2025 AT 08:28They’re hiding this. Big Pharma knows. That’s why azithromycin is pushed so hard. It’s cheaper. And they don’t want you knowing how dangerous the others are. Your doctor’s EHR doesn’t warn you because they’re paid to keep you on the risky ones.
Jimmy Jude
December 10, 2025 AT 10:57It’s not the drug. It’s the system. We treat pills like candy, and then act shocked when the universe bites back. Colchicine is ancient wisdom. Macrolides are modern arrogance. When you ignore the body’s quiet signals-because you’re too busy scrolling-you’re not just risking death. You’re disrespecting evolution itself.
Juliet Morgan
December 11, 2025 AT 06:58OMG I just realized my grandpa’s on both of these… I’m calling his doctor right now. Thank you for posting this. I was so scared after reading the stats. Please keep sharing stuff like this. 💙
Harry Nguyen
December 12, 2025 AT 11:35So let me get this straight-you’re telling me that because I take colchicine for gout, I can’t take antibiotics for a cold? What’s next? No ibuprofen? No coffee? Next you’ll say we should all live in caves and eat raw kale. This is why medicine is broken. Everyone’s terrified of a single pill.
Katie Allan
December 14, 2025 AT 01:21This is one of the most important posts I’ve read all year. Thank you for the clarity, the data, and the actionable steps. We need more of this-no fluff, just facts, and a roadmap. I’m sharing this with my entire family and my book club. Knowledge is the first real protection we have.
Deborah Jacobs
December 14, 2025 AT 08:57I used to think colchicine was just that weird little pill my aunt took for her ‘bad joints.’ Then she ended up in the hospital after her pneumonia meds. She didn’t even know it was colchicine-thought it was a vitamin. I cried for days. Now I check every med my family takes like it’s a bomb squad. You don’t need a degree to save a life. Just curiosity.
James Moore
December 15, 2025 AT 06:51Let’s be real here-the entire pharmaceutical-industrial complex is built on obfuscation. The fact that CYP3A4 inhibition by macrolides has been documented since the 1980s but only now is there a tiered alert in Epic? That’s not negligence. That’s profit-driven inertia. And the fact that genetic testing for ABCB1 variants is still considered "emerging" when it’s been validated in peer-reviewed journals since 2020? That’s systemic malpractice wrapped in white coats.
Kylee Gregory
December 15, 2025 AT 13:42I’m a nurse and I’ve seen this happen twice. One patient was 78, on colchicine for pericarditis, got clarithromycin for bronchitis. Got rhabdomyolysis. We caught it in time because his daughter asked why he was so weak. But what about the ones who don’t have advocates? We need mandatory pharmacist counseling when colchicine is prescribed. Not optional. Mandatory.
Carole Nkosi
December 15, 2025 AT 20:43Why is this even a conversation? In my country, we don’t mix these drugs. We use alternatives. The fact that you’re still debating this means your healthcare system is broken. People are dying because you’re too slow to fix what’s obvious.
Stephanie Bodde
December 16, 2025 AT 01:10My mom is on colchicine and just got azithromycin last week! I was so nervous but she asked the doc and they switched right away 😌 Thank you for the heads-up! I’m printing this out for my aunt too!
Philip Kristy Wijaya
December 16, 2025 AT 23:27Jennifer Patrician
December 17, 2025 AT 01:27They’re testing this on us. The FDA, the CDC, the AMA-they all know this interaction kills. But they’re letting it happen to make room for COL-098. That’s the real drug. The one they’ll charge $10,000 a year for. This isn’t a warning. It’s a marketing campaign. Wake up.